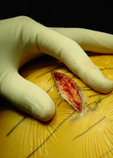
A 3-inch incision is made in the side of the hip and the muscles are moved aside to reach the joint and allow the implants to be easily placed. The mini-posterior method works by dislocating the hip towards the back of the body. This method, combined with the use of special surgical instruments, significantly decreases the risk of postoperative limping, nerve damage, and other complications.